Tandem Diabetes Care ProductsCreating New Possibilities for People Living with Diabetes
We know that diabetes management is a personal journey to keep blood glucose balanced throughout the day and night. That’s why we deliver innovative insulin pumps, automated insulin delivery systems, supplies, and technology.
Choose a Pump

Tandem Mobi System
Impressively small and can be worn almost anywhere,* Tandem Mobi gives you more options for how you manage your diabetes.
Available Features
![]() Powered by Control-IQ+ technology
Powered by Control-IQ+ technology
![]() Capable of remote software updates†
Capable of remote software updates†
![]() Smartphone control (iOS & Android)‡
Smartphone control (iOS & Android)‡
![]() Holds 200 units of insulin
Holds 200 units of insulin
![]() Pump button for bolus delivery
Pump button for bolus delivery
Dexcom sensor compatibility§
![]() Inductive wireless charging
Inductive wireless charging
![]() On-body wear with adhesive sleeve^
On-body wear with adhesive sleeve^
t:slim X2 Insulin Pump
With a sleek color touchscreen, this all-in-one insulin pump integrates seamlessly into your life like a sophisticated, modern device.
Available Features
![]() Powered by Control-IQ+ technology
Powered by Control-IQ+ technology
![]() Capable of remote software updates†
Capable of remote software updates†
![]() Mobile bolus delivery (iOS & Android)‡
Mobile bolus delivery (iOS & Android)‡
![]() Holds 300 units of insulin
Holds 300 units of insulin
![]() Pump button for bolus delivery
Pump button for bolus delivery
Dexcom sensor compatibility§
![]() FreeStyle Libre 3 Plus sensor compatibility
FreeStyle Libre 3 Plus sensor compatibility
![]() Integrated color touchscreen
Integrated color touchscreen
Order a Tandem Diabetes Care Automated Insulin Delivery System Today.
A Tandem Diabetes Care Specialist will help you get started.

Tandem Diabetes Care #1 Favorite Pump
You may be able to experience the life-changing benefits of Tandem automated insulin delivery for $0 out of pocket.
Check BenefitsSeagrove PWD Survey: Nov. 2024.
Cost per day calculation reflects the average monthly out-of-pocket cost for pump and disposables necessary to utilize Tandem pump therapy over the life of the 48-month pump warranty. Assumes consumption of 10 infusion sets and cartridges per month.
$0 out of pocket claim based on direct orders from Tandem customers with commercial insurance from 1/1/2025-12/31/2025. Data on file. Actual cost may vary and is subject to individual insurance coverage.
Choose an Infusion Set
Disconnect. Reconnect. It’s a Snap!
Finding the right infusion set is an important part of successful insulin pump therapy. Choose from different insertion angles, materials, and a variety of a tubing lengths.

Discover Innovative Tools
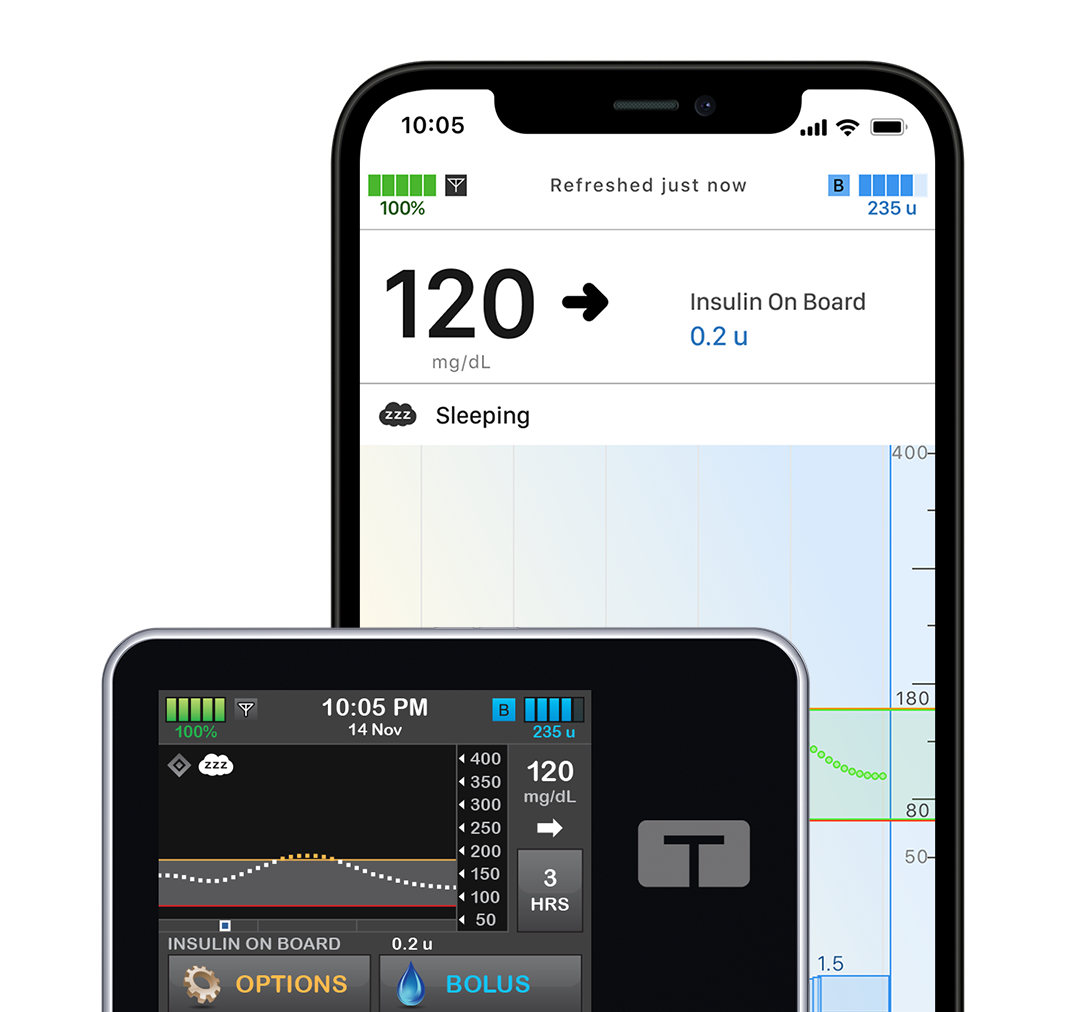
Connected Care System
We are more than an insulin pump company. We also support users through cutting-edge mobile and cloud-based applications that are designed to help you see therapy data and better manage your diabetes.

Choose Pump Accessories
Personalize Your Pump
We know that your insulin pump is an integral part of your life. That’s why we offer a wide range of pump accessories for wearability, power sources, and protection that meet your needs.
